
Pulmonary Hypertension (PH) is a serious and progressive condition where the blood pressure in the arteries of the lungs becomes abnormally high. Over time, this extra pressure forces the right side of the heart to work much harder than normal. If untreated, it can eventually lead to right heart failure.
Although it is not as commonly discussed as systemic hypertension (high blood pressure in the body), pulmonary hypertension can carry significant health risks and requires early recognition and proper management.
What Is Pulmonary Hypertension?
Pulmonary hypertension is defined as a condition where the mean pulmonary artery pressure (mPAP) exceeds 20 mmHg at rest. This measurement is usually confirmed through a procedure known as right heart catheterization, which is considered the gold standard diagnostic test.
The disease increases resistance in the pulmonary circulation, forcing the right ventricle of the heart to pump harder in order to push blood into the lungs.
- Mean Pulmonary Artery Pressure (mPAP): >20 mmHg at rest
- Pulmonary Vascular Resistance (PVR): ≥2 Wood units
- Pulmonary Artery Wedge Pressure (PAWP): used to distinguish between different types of pulmonary hypertension
Types of Pulmonary Hypertension
The World Health Organization (WHO) classifies pulmonary hypertension into five major groups based on underlying causes.
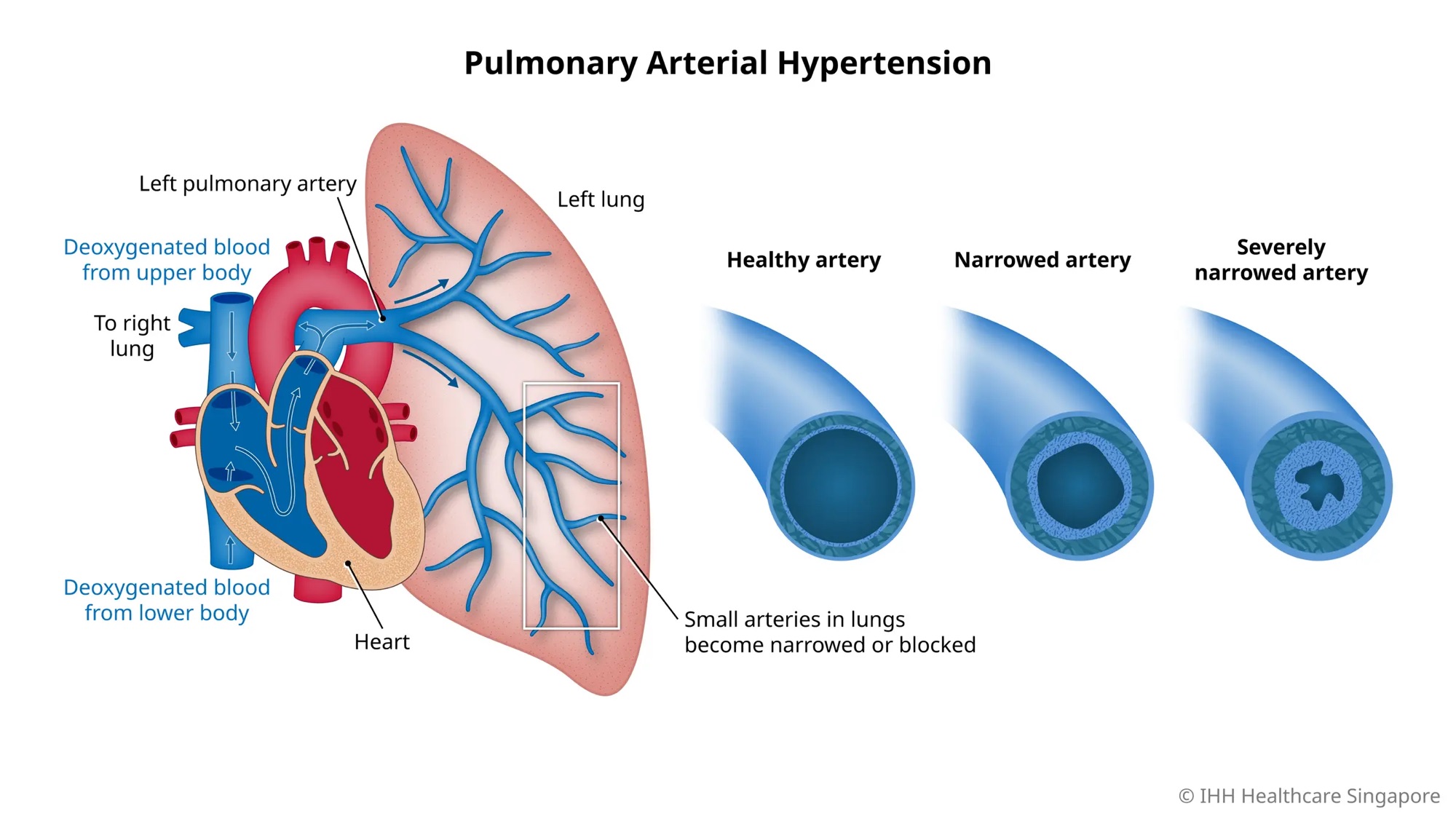
Group 1: Pulmonary Arterial Hypertension (PAH)
- Idiopathic (unknown cause)
- Genetic or heritable forms
- Drug-induced cases
Group 2: PH Due to Left Heart Disease
This is the most common cause of pulmonary hypertension and results from conditions affecting the left side of the heart.
Group 3: PH Due to Lung Disease or Hypoxia
- Chronic Obstructive Pulmonary Disease (COPD)
- Interstitial Lung Disease (ILD)
- Long-term oxygen deficiency
Group 4: Chronic Thromboembolic Pulmonary Hypertension (CTEPH)
This occurs when blood clots obstruct pulmonary arteries and increase pressure in the lung circulation.
Group 5: Multifactorial or Unclear Causes
Some cases develop due to complex or poorly understood mechanisms.
Causes and Risk Factors
Pulmonary hypertension can develop from several underlying medical conditions.
- Connective tissue disorders such as systemic sclerosis
- Congenital heart disease with abnormal blood flow
- Chronic lung diseases
- Obstructive sleep apnea
- Portal hypertension (liver disease)
- HIV infection
- Certain medications, including appetite suppressants
What Happens Inside the Body?
Pulmonary hypertension involves several pathological changes in the pulmonary arteries.
- Damage and dysfunction of the endothelial lining of blood vessels
- Reduced production of nitric oxide and prostacyclin, which normally help blood vessels relax
- Increased endothelin-1, causing blood vessel constriction
- Thickening and remodeling of pulmonary artery walls
These changes gradually increase resistance in the lung circulation. As the pressure rises, the right ventricle enlarges and thickens in an attempt to compensate. Eventually, this can lead to right-sided heart failure.
Common Symptoms
Early symptoms can be subtle and are often mistaken for general fatigue or lung problems.
- Shortness of breath during physical activity
- Persistent fatigue
- Chest discomfort or chest pain
- Dizziness or fainting (syncope)
- Swelling in the legs or ankles
- Abdominal swelling due to fluid buildup (ascites)
Doctors may also detect a loud P2 heart sound during a physical examination.
How Is Pulmonary Hypertension Diagnosed?
Diagnosis usually involves several tests to confirm the condition and identify its cause.
- Echocardiography – the first non-invasive screening test
- Right heart catheterization – confirms diagnosis and measures pressures
- Electrocardiogram (ECG) – may show right ventricular strain
- Chest X-ray – can reveal enlarged pulmonary arteries
- Blood tests (BNP or NT-proBNP) – help assess heart strain and prognosis
Treatment and Management
Treatment depends on the underlying cause and severity of the disease. Management often includes both supportive care and targeted medications.
General Supportive Care
- Oxygen therapy
- Diuretics to reduce fluid buildup
- Anticoagulants in selected patients
- Lifestyle modifications and supervised exercise
Targeted Medications
- Endothelin receptor antagonists – Bosentan, Ambrisentan
- Phosphodiesterase-5 inhibitors – Sildenafil, Tadalafil
- Prostacyclin analogues – Epoprostenol, Iloprost
- Soluble guanylate cyclase stimulators – Riociguat
In severe cases that do not respond to medical treatment, lung transplantation may be considered.
Complications and Prognosis
Without treatment, pulmonary hypertension can progressively worsen and lead to life-threatening complications.
- Right-sided heart failure
- Cardiac arrhythmias
- Blood clots in the lungs
The outlook for patients varies depending on the underlying cause, disease severity, and how well they respond to therapy. Early diagnosis and modern combination treatments have significantly improved survival rates.
Final Thoughts
Pulmonary hypertension is a complex but manageable condition when detected early. Recognizing symptoms such as unexplained shortness of breath and fatigue is important. With proper medical care, targeted treatments, and regular monitoring, many patients can maintain a better quality of life.
![]()

